Palate Expander Adults What is actually possible, & what is not.
Most adults are told palate expansion is only for children, that the bones have fused and nothing can be done. That is not the whole story. Adult palate expansion is possible, but it requires a different approach, a structural diagnosis, and an honest conversation about what the evidence supports.
The narrow palate problem does not disappear when you turn 18.
Adults present at the clinic with the same structural problem children do, except they have lived with it longer. A narrow upper jaw, crowded teeth, mouth breathing, snoring, jaw clicking, fatigue. The cluster is the same. The biology underneath is different, which is why the treatment has to be too.
The "you're too old" response from general dentists is rarely wrong about the standard tools. It is usually wrong about what is currently possible.
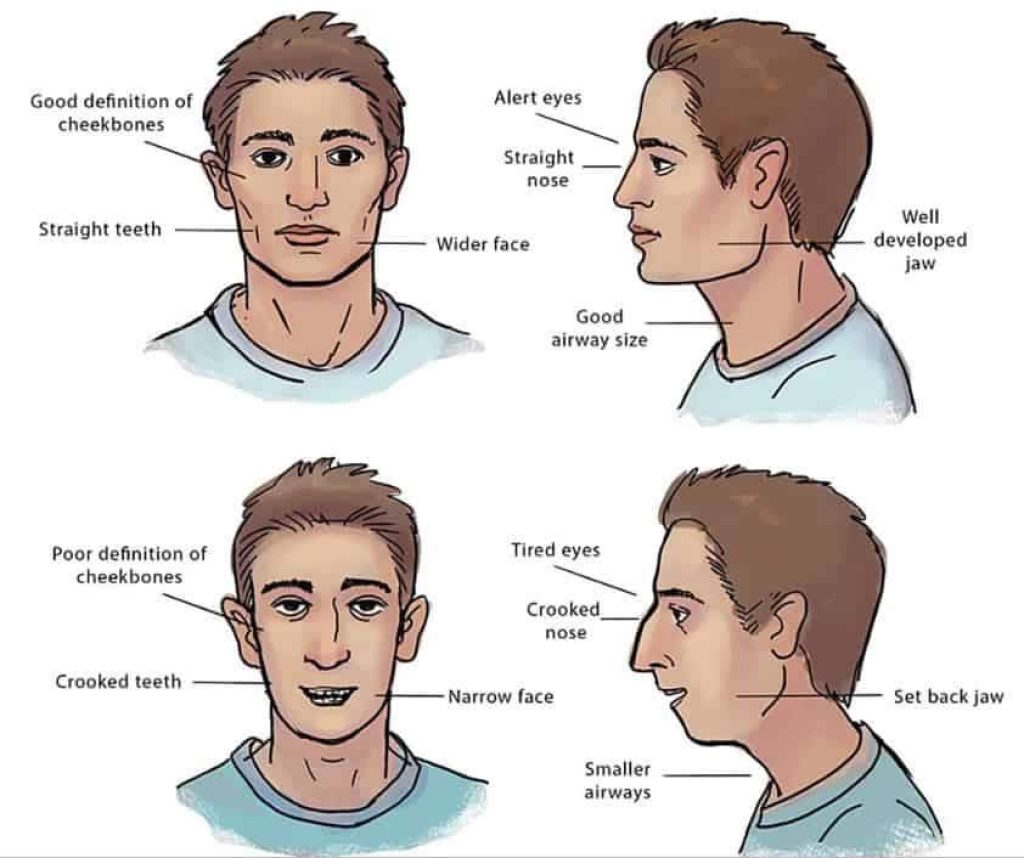
What a narrow palate is actually doing to your airway.
Run your tongue along the roof of your mouth. That bone is the floor of the nasal cavity above and the ceiling of the space the tongue rests in below. A narrow high-vaulted palate reduces room in both directions. The tongue often falls back during sleep, the upper airway loses volume, and the symptoms cluster the way they do.
This is the chain. Naming it changes how the rest of the page reads.
Why adult expansion is harder, but not impossible.
The mid-palatal suture, the join along the centre of the upper jaw, fuses gradually. The textbook range is wide and individual variation is significant. Some adults retain meaningful suture activity into their thirties. Others fuse earlier. CBCT imaging is the only honest way to know your specific situation.
What changes in adults is the device and the protocol, not the possibility. The structural goal is the same; the route to it is different.
A useful way to think about this: in children, the suture is a hinge; in adults, it is more like a seam. Both can be opened, but the seam needs different tools and a different rate. The seam can also be in different states of fusion at the front versus the back, which is why imaging matters more in adults than in growing children.
The devices used for adult palate expansion, and how they differ.
- MARPE (Miniscrew-Assisted Rapid Palatal Expander). Titanium miniscrews drive expansion force into the palatal bone via skeletal anchorage. Often the right choice for adults where conventional expanders would just tip teeth outward.
- MSE (Maxillary Skeletal Expander). A close relative of MARPE, also bone-anchored, used interchangeably in much of the literature.
- Tooth-borne expanders. Lighter forces, faster to fit, generally insufficient alone in adults because the suture resists.
- SARPE. Surgically Assisted Rapid Palatal Expansion. Reserved for cases where the suture is fully fused and non-surgical approaches are not viable.

What the clinical evidence says about adult expansion.
The literature on adult bone-anchored expansion has grown substantially in the last ten years. Studies on MARPE consistently report that meaningful skeletal expansion is achievable in adult patients, with the size of the gain varying by suture maturity, bone quality and protocol. Success rates in published series are typically reported between 80 and 90 percent in appropriately selected cases.
The literature on slow expansion in adults is less standardised because the protocols vary more between practices, but our clinical experience and that of colleagues using comparable approaches suggests outcomes that are competitive with rapid protocols and often more comfortable for patients.
No clinical evidence is a substitute for a CBCT scan of your specific anatomy. We mention the evidence because patients sometimes arrive having read social-media confidence dressed up as fact, and the honest version sits between optimism and dismissal.
What the outdated approach looks like, and why it often made things worse.
Extraction-based orthodontics. Remove premolars, retract the remaining teeth backward to relieve crowding. Fast and predictable.
In adults whose jaws were already narrow, this approach often reduced the arch further and pushed the dentition further back, taking space from the tongue and the airway. The patient who comes to the clinic in their thirties asking about snoring and fatigue, having had extractions as a teenager, is the textbook case. We are not assigning blame, just explaining the pattern.
The WideSmiles™ approach to adult jaw expansion.
WideSmiles™ is the slow-expansion method we use within Jawthodontics™. Where MARPE is the right call we use it. Where slow expansion can achieve the same skeletal change with less invasiveness, we use that instead. The protocol is personalised to your suture status, your airway picture, and your goals.
The point is not to win a faster timeline. The point is a result that holds.
Coordinated care: who else we work with.
Adult expansion rarely lives in isolation. The structural change in the upper jaw affects the way the tongue rests, the way you breathe at night, and the way the rest of the mouth aligns. Coordinated care with other clinicians is part of how the work holds.
Myofunctional therapists retrain the tongue and orofacial muscles to use the new space the expansion creates. Sleep doctors evaluate airway-related symptoms before and after expansion when sleep-disordered breathing is part of the picture. ENT colleagues address any structural nasal obstruction (deviated septum, enlarged turbinates) that expansion alone will not resolve. We have a small network of practitioners in London we work with regularly.
The coordination is part of the plan, not an afterthought. You will know about any onward referrals before treatment begins, and you will not be left to construct the team yourself.
What the NHS does and does not cover for adults.
NHS orthodontic treatment for adults is very limited and palate expansion for adults is not routinely offered. Most adults seeking this treatment will need to access it privately. We are stating this without editorialising.
What to expect: timeline, process, and realistic outcomes.
Active expansion runs over several months, with the device activated on a defined schedule. A retention phase follows so the new bone in the suture can consolidate. Adult timelines tend to be longer than childhood timelines.
Outcomes may include a wider arch, more tongue space, increased nasal airway volume in some cases, reduced crowding, and changes in lower-face support that are usually subtle in adults. None of these is guaranteed; all are the rationale for the work.
The day-to-day of living with the device.
For the first three to seven days, the device is the most noticeable thing in your mouth. Speech can feel slightly different (most patients adjust within a week), eating takes more chewing on softer foods, and the tongue is busy investigating an unfamiliar surface on the roof of the mouth. By the end of the second week, most patients report that the device feels unremarkable most of the time.
Activations (the small turns of the screw that drive the expansion) usually happen once or twice a day on a defined schedule. Each activation is brief and painless to perform, though many patients describe a pressure sensation in the upper face and around the nose for the next hour or two. The pressure settles as the bone adapts.
A small temporary gap between the upper front teeth is normal during active expansion. It is a sign the suture is opening, not a problem, and it closes as the surrounding teeth and bone settle. Patients sometimes find this aesthetically unsettling at first. We show photos of the predictable trajectory so it does not arrive unannounced.
Who we say no to, and why that matters.
Adult palate expansion is not appropriate for every adult who asks about it. CBCT findings rule some patients out: a fully and densely fused suture in an older patient with thin palatal bone is not a sensible candidate for MARPE, and the honest answer in that case is either surgical SARPE or no expansion at all.
Some adults arrive convinced that expansion will resolve a symptom that has a different cause. Severe obstructive sleep apnoea is not a condition that palatal expansion alone is designed to treat. Significant nasal airway obstruction from a deviated septum or enlarged turbinates needs ENT input that expansion alone cannot replace. We will refer onward, not treat in-house, when those are the dominant findings.
We say no because the alternative (treating patients who do not need the work or who will not benefit from it) is the failure mode that makes a clinic untrustworthy. A clear no, given early, is more valuable than a polite yes that costs you a year.
Is adult palate expansion right for you?
Age, symptoms, airway involvement, bone structure, treatment goals. Those five variables decide. A pre-consultation can map them in fifteen minutes. The full assessment can answer them with imaging.
Frequently asked
Can adults really use a palate expander?
Yes, in many cases adults can undergo palate expansion, though the approach differs from treatment in children or teenagers. Bone-anchored devices such as MARPE may be used when the mid-palatal suture has become more resistant to conventional expansion. A structural assessment, often including 3D imaging, can help determine what is possible for your specific anatomy.
At what age is it too late for palate expansion?
There is no single cut-off age. The mid-palatal suture typically becomes more resistant to expansion in the late teens and early twenties, but individual variation is significant. Adults in their 30s and 40s may still be candidates for bone-anchored expansion, depending on bone density and clinical goals. A proper structural diagnosis is the only reliable way to know.
Does palate expansion help with sleep apnoea or snoring in adults?
Widening the palate can increase tongue space and may reduce airway restriction in some adults. This does not mean expansion is a treatment for sleep apnoea, and outcomes vary. If airway symptoms are part of the picture, a clinician who takes an airway-first approach is better placed to assess whether expansion is appropriate alongside other interventions.
Is palate expansion available on the NHS for adults?
NHS orthodontic treatment for adults in the UK is very limited, and palate expansion for adults is not routinely offered. Most adults seeking this treatment will need to access it privately. A pre-consultation can help clarify what is involved and whether it is appropriate for your situation.
How long does adult palate expansion take?
Treatment timelines vary depending on the device used, the degree of expansion needed and individual biology. Adult expansion often takes longer than adolescent treatment and may be followed by a retention phase. Your clinician should give a realistic timeline based on your specific case.
What is the difference between a removable palate expander and a fixed one for adults?
Removable expanders rely on the patient wearing them consistently and are generally considered less effective for adults with more resistant bone. Fixed bone-anchored devices such as MARPE apply controlled force directly to the palate and are often preferred for adults where meaningful skeletal expansion is the goal. The right choice depends on your anatomy and what you are trying to achieve.
Will palate expansion change the appearance of my face?
Widening the upper jaw can have subtle effects on facial appearance, including a broader smile and potentially improved lip support. These changes are usually modest in adults and should not be the primary reason for treatment. The structural and airway benefits are the more clinically meaningful goals.