Palate Expander UK What it is, who needs one, & why the jaw width question matters more than most dentists explain.
Most people think of a palate expander as a children's brace that creates room for crowded teeth. The structural truth is more important: the roof of the mouth is also the floor of the nose, so a jaw that never widened properly does not only crowd the teeth, it can quietly compress the airway for life.
The palate is the floor of your nose, and the ceiling of your airway.
Open your mouth and put a finger on the roof. That thin shelf of bone is the floor of your nasal cavity above and the upper boundary of the space your tongue lives in below. When the palate is narrow and high-arched, three things tend to happen at once: the nose has less room to breathe through, the tongue is pushed down and back, and the upper teeth have nowhere to sit except crowded.
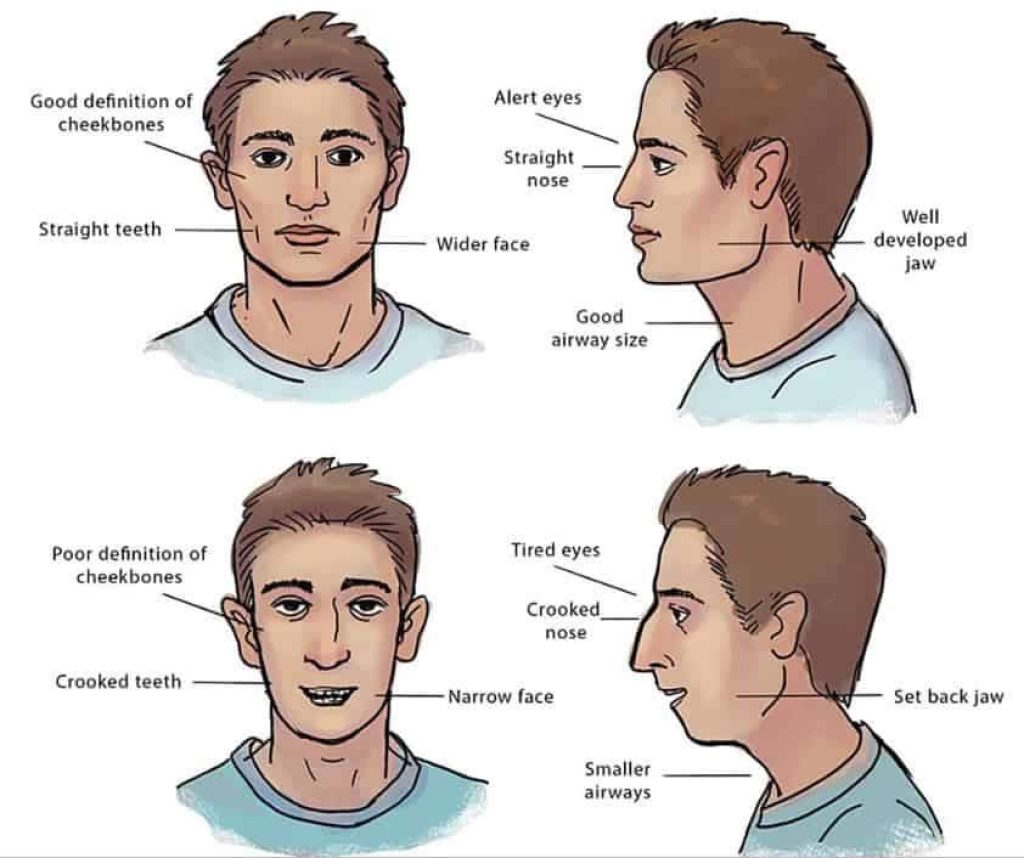
This is the chain that turns a structural question into a breathing one. A narrow palate is not just a dental inconvenience. It is the upstream cause of symptoms most patients have been told are unrelated to their jaw at all: mouth breathing, snoring, broken sleep, grinding, jaw clicking, a face that looks compressed. In an airway-first practice, palate expansion is not a cosmetic procedure. It is structural work on the foundation everything else sits on.
What a palate expander actually does inside the bone.
A palate expander is not a brace that pushes teeth. It is a device that applies slow, controlled lateral force at the midline of the upper jaw, where the two halves of the palate meet at the mid-palatal suture. In a young, unfused suture the force gradually separates the two halves and new bone fills the gap as the body remodels. This is skeletal expansion, not tooth movement.
The visible signs during treatment can be unsettling if you have not been warned: a small gap can appear between the upper front teeth as the suture opens. That diastema is a feature of the mechanism working, not a problem. It typically closes on its own as the surrounding teeth and bone settle. The bone that fills the suture takes longer to consolidate than the visible gap takes to close, which is why a retention phase is always part of the treatment plan.
How quickly the suture responds depends on age, anatomy and force protocol. There are several appliance categories in use:
- Removable plates and quad-helix devices, generally for younger children with very compliant biology.
- Fixed Rapid Palatal Expanders (RPE) bonded or banded to the upper teeth. The standard option through adolescence.
- Bone-anchored devices such as MARPE (Miniscrew-Assisted Rapid Palatal Expansion), which deliver force directly into the palatal bone via small titanium miniscrews. This is the option that often makes adult expansion possible without surgery.
The signs your jaw may be too narrow.
None of the following on its own is a diagnosis. Taken together, they are the cluster we see again and again at the clinic in patients who turn out to have a narrow upper arch. They are signals worth taking seriously, not a checklist to self-diagnose from.
- Crowded upper teeth, or teeth that needed extracting to fit.
- A high-arched palate that feels like a narrow vault when you run your tongue across it.
- Habitual mouth breathing during the day, or a dry mouth on waking.
- Snoring, restless sleep, or a partner who has noticed pauses in breathing.
- Grinding (bruxism) or daytime jaw clenching.
- A history of tongue tie, even one previously dismissed as mild.
- Forward head posture, persistent low-grade fatigue, or a feeling that the lower face is recessed.
Modern human jaws are smaller compared to our ancestors. Jaw expansion aims to put nature back on track.
Children versus adults: the options are different, not unavailable.
The most common piece of misinformation we hear from new adult patients is that they were told expansion is "only for children". The honest version is that the approach changes with age, not that the option disappears.
The mid-palatal suture fuses gradually through adolescence and early adulthood. The textbook range is wide. Fusion often progresses through the late teens and twenties, but timing varies significantly between individuals. In children, a removable or fixed conventional expander typically works well because the suture is still open and responsive. In adults, the bone resists the same force, and pushing tooth-borne devices harder generally tips the teeth outward rather than widening the skeleton.
This is why MARPE exists. By anchoring the expansion force into the bone of the palate itself, rather than the teeth that sit on it, MARPE can achieve skeletal change in many adults whose sutures have begun or completed fusion. Where the suture is fully and densely fused, a surgical option called SARPE (Surgically Assisted Rapid Palatal Expansion) may be discussed. None of this is guaranteed without imaging. A CBCT scan is the only reliable way to assess suture status in an individual.
On the question almost every UK reader is also asking: conventional palate expansion for children may be available on the NHS in cases that meet orthodontic need criteria (assessed under the Index of Orthodontic Treatment Need). Adult skeletal expansion is almost universally a private treatment in the UK. We say this without editorialising. It is the practical reality, and our job is to help you decide what to do about it.

The outdated approach: extraction to make space.
For most of the last century, the conventional orthodontic answer to a crowded upper arch was straightforward: remove premolars to create room, then retract the remaining teeth back into the gap. It produces straighter front teeth in a predictable timeframe, which is why it became the default. The structural cost is rarely discussed.
Extracting and retracting reduces the perimeter of the upper arch. The teeth move backwards, the tongue has less room to occupy than it did before, and the soft palate at the back of the mouth has less space to sit forward of the airway. We are not claiming that every extraction case causes harm. We are saying that the choice should be made with the airway in mind, not in isolation. Patients who had teeth removed as teenagers and are now in their thirties asking us about snoring, fatigue and a sense of facial compression are not imagining a connection.
How WideSmiles™ approaches palate expansion at the clinic.
WideSmiles™ is the expansion method we use within the broader Jawthodontics™ framework. The shorthand version: structure first, airway always, teeth last. Every treatment plan is built around three things the appliance itself cannot change: the maturity of your suture, the dimensions of your airway and the relationship between your upper and lower jaw. Only then do we choose which device delivers the force the bone needs.
For a child or younger teenager, that often means a conventional fixed expander followed by retention and, where indicated, downstream alignment. For an adult, it more often means MARPE alongside an honest conversation about what the imaging shows. In a small number of cases, the right answer is to refer for a surgical opinion rather than treat in-house. We will say so plainly if that is what your scan suggests.
What the assessment process in London actually involves.
A structural jaw assessment is not a standard orthodontic consultation. We are not measuring whether your teeth are crooked. We are measuring whether the bones that house them are the right size for the airway above them.
The full diagnostic appointment runs sixty minutes and includes a CBCT scan to map the suture, the airway and the jaw joints in three dimensions; a clinical evaluation of tongue posture and breathing pattern; a review of any prior orthodontic history including extractions; and an unhurried conversation about which symptoms brought you in and which you have stopped noticing because you have lived with them too long. The assessment fee is £350, and it is fully redeemable against treatment if you choose to proceed.
If after the assessment we do not think expansion is the right answer for your specific case, we will say so. The whole approach falls apart if we treat patients who do not need it.
Common questions about palate expanders in the UK.
The questions below are the ones we are asked most often by readers who land on this page. Full FAQ answers are in the panel below. If your situation does not quite fit any of them, please write to us at concierge@drdepen.com. We would rather answer in detail than leave you wondering.
Frequently asked
Can adults get a palate expander in the UK?
Adults can often benefit from palate expansion, though the approach differs from childhood treatment. Once the mid-palatal suture has fused, a technique called MARPE (Miniscrew-Assisted Rapid Palatal Expansion) may be used to achieve skeletal widening. Suitability depends on individual bone quality and airway assessment, and a CBCT scan is the reliable way to know.
Is a palate expander available on the NHS?
Conventional palate expanders for children may be available through NHS orthodontic treatment in some cases, depending on clinical need as assessed by the Index of Orthodontic Treatment Need. Adult skeletal expansion is almost always provided privately in the UK, as it falls outside standard NHS orthodontic provision.
How long does palate expansion take?
Treatment timelines vary depending on the individual, the device used, and the degree of expansion needed. In children, active expansion may take several months, followed by a retention period. Adult MARPE protocols also commonly run for several months of active expansion, with consolidation time built in to allow the bone in the suture to mature.
Does a palate expander help with breathing or snoring?
Widening the palate may increase nasal airway volume and improve tongue posture during sleep, which can in some cases reduce mouth breathing and snoring. The relationship between jaw structure and airway is well-established, though individual outcomes vary and a structural assessment is needed to determine whether expansion is likely to help in your specific case.
At what age should a child get a palate expander?
Early intervention is often easier because the mid-palatal suture is still open and responsive to gentle force. Many clinicians consider the window between ages 7 and 14 to be particularly favourable, though this depends on the child's development. A structural assessment can help determine the right timing for your child specifically.
What is the difference between a palate expander and braces?
Braces move teeth within the existing jaw structure. A palate expander works on the bone itself, widening the arch to create more space. In an airway-first approach, expansion is often considered before or alongside any tooth alignment work, because the structural foundation affects everything above it.
Will a palate expander change the shape of my face?
Palate expansion may produce subtle changes in facial width and nasal appearance in some cases, particularly in younger patients whose bones are still developing. Adult changes tend to be more modest. Any visible changes are a secondary effect of the structural work, not a cosmetic goal.