Adult Tongue Tie Release UK What nobody tells you about the structural picture.
Most adults with tongue tie are told it is a baby problem, or that they have already adapted, or that the NHS will sort it. The structural picture is more complicated. A restricted frenum limits tongue posture, which limits jaw development, which limits airway space. The symptoms that follow are rarely traced back to their source.
The symptom list that keeps getting ignored.
Difficulty elevating the tongue. Jaw tension. Forward head posture. Mouth breathing. Disrupted sleep. Speech that feels effortful even though it is fluent. A swallow that does not feel quite right. A lisp that never fully resolved.
These are the presentations that bring most adults here. None of them are diagnostic on their own. Together they describe a pattern that is hard to fit into a single specialty's remit, which is why most adults living with them have been to several clinicians and left without a name for what was going on.
What tongue tie actually is in an adult jaw.
The lingual frenulum is a fold of tissue under the tongue. When it is tight or attached too far forward, the tongue cannot elevate or extend freely. In an adult, that restriction has been shaping where the tongue rests, how the swallow works, and how the jaw developed for decades.
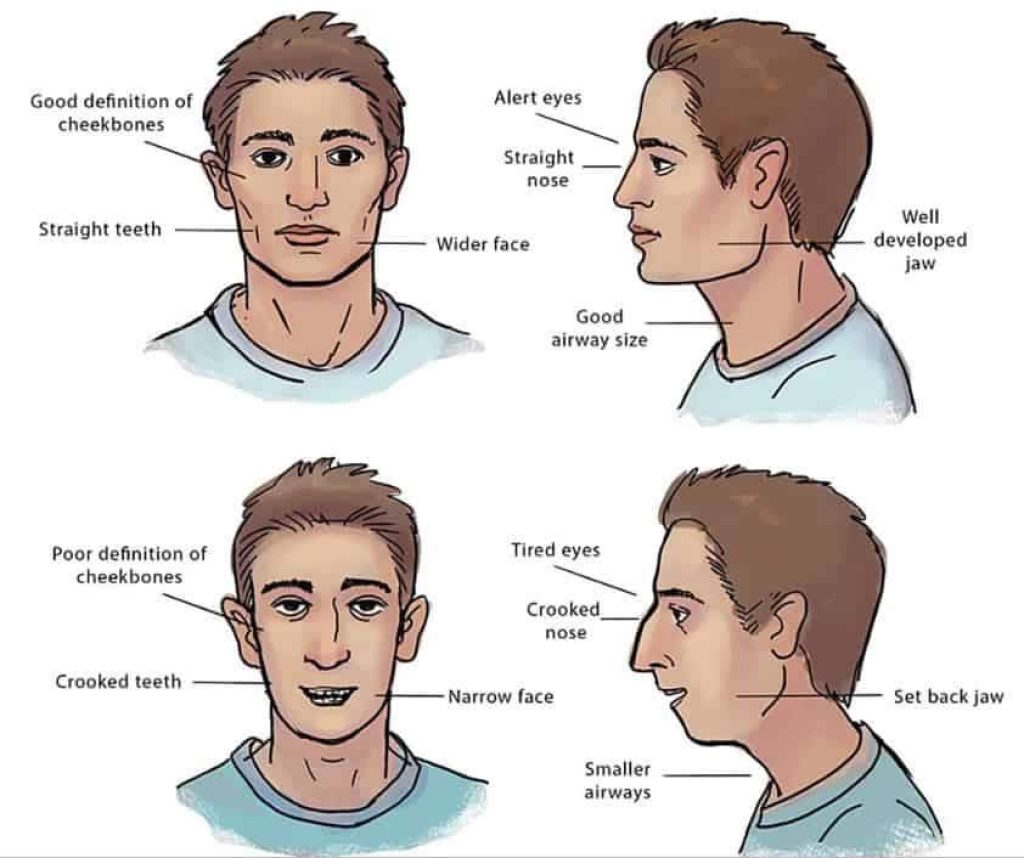
The tongue is also the body's natural palatal expander. When it rests against the roof of the mouth, it provides upward pressure that helps maintain palate width. A tongue that cannot reach the palate cannot perform that role. Over years, the arch tends to narrow, the palatal vault tends to rise, and the airway above tends to lose volume.
Why most adults were never diagnosed.
Posterior tongue tie, the submucosal variety, is frequently missed on visual inspection. It can look normal under a torch but feel restricted on examination. Classification systems vary between practitioners, and none is universally agreed upon.
Many adults were assessed as infants using criteria designed to predict breastfeeding success, not structural development. A baby who fed adequately on a partial release was rarely followed up. The structural cost did not become visible until much later.
The link between tongue tie and a narrow jaw.
The tongue at rest is meant to sit against the palate. A restricted frenum prevents that. The tongue rests lower and forward, the palate misses the developmental pressure it needs, and the arch comes in narrower than it would otherwise.
The downstream consequences accumulate. A narrower arch crowds the teeth and reduces room for the tongue itself. The tongue often falls further back during sleep. The airway loses volume. The symptoms become harder to trace because they look like several separate problems rather than one upstream cause.
What the procedure involves for adults in the UK.
Frenotomy is a small release using scissors or laser, performed under local anaesthetic. Frenectomy is a fuller release that removes a wedge of tissue. The technique chosen depends on the anatomy and the goal of the release.
NHS provision for adult tongue tie release is very limited in the UK and largely focused on infants. Most adults seeking release will need to self-fund. Wound care, follow-up exercises and myofunctional rehabilitation matter as much as the cut itself, and these are rarely included in low-cost release-only packages.
The procedure itself runs around thirty to forty-five minutes once the assessment work is complete. Local anaesthetic is used. The release is performed with either scissors or a diode laser depending on the anatomy and the goal. Most adults eat softer food for forty-eight to seventy-two hours afterwards and return to normal speech and eating within one to two weeks.
Laser versus scissor release: does it matter?
There is no settled clinical evidence that one technique is universally superior to the other. The internet often presents this as a controversy; in practice it is a tool choice that depends on the anatomy and the operator.
Diode laser release tends to produce less bleeding, can be more precise in posterior tongue tie cases, and may shorten recovery in some patients. Scissor release is straightforward, requires no specialised equipment, and is the long-standing technique. Either method, performed competently and followed by appropriate aftercare and rehabilitation, can produce a good outcome.
We use what suits the case in front of us. The technique matters less than the planning that precedes it and the rehabilitation that follows.
Why release without rehabilitation often underdelivers.
The frenum has been restricting tongue movement for decades. The muscles around it have adapted to that restriction. Cutting the tissue changes the anatomy; it does not retrain the function. Without myofunctional rehabilitation, many adults find the tongue does not adopt a correct rest posture even after a successful release.
A release without a rehab plan is half a treatment. We would rather refer to a myofunctional therapist for several sessions before considering the cut than do a release without that support in place.
What aftercare actually involves.
The first two weeks after release matter more than the procedure itself. Wound care is straightforward: gentle stretching exercises through the day to discourage the tissue from reattaching too tightly, basic oral hygiene, and over-the-counter pain relief as needed. The stretches are uncomfortable for the first few days and easier after that.
Myofunctional exercises typically begin within the first week, once the initial soreness has eased. Your therapist will guide the schedule. The combination of stretching (to maintain the new anatomical range) and myofunctional work (to retrain the muscular function) is what protects the result.
We will see you for a follow-up at two weeks to assess healing, and again at six weeks to check that tongue function is moving in the right direction. If something is not progressing as expected, we adjust the plan early rather than waiting.
What adult tongue tie release typically costs in the UK.
Adult release is rarely available on the NHS, so this is almost always a private decision. Prices vary widely between providers, which is consistent with the variation in what is actually included. A release-only package at a low price often excludes the structural assessment, the myofunctional rehabilitation, and the follow-up that determine whether the result holds.
We do not publish a treatment-fee menu on this page because the right approach depends on the assessment. What we will say is that the £350 Jaw & Airway Analysis is the only price you will see on this site for diagnostic work, and it is fully redeemable against treatment if you proceed.
What a realistic outcome looks like.
Adult tongue tie release done well, with appropriate expansion where indicated and consistent myofunctional rehabilitation, can produce meaningful changes. Tongue mobility improves. Resting tongue posture often shifts up to the palate over months. Jaw tension and clenching can ease. Sleep quality may improve in cases where the airway was part of the structural picture.
None of this is guaranteed, and the timeline is months rather than weeks. Adults sometimes expect to feel different the day after the procedure. The cut is the smaller part of the work; the muscular retraining and the bone biology around it are what produces the result. We say this on the first visit so the expectation is calibrated before treatment begins.
Outcomes are most predictable when the patient does the rehabilitation work between appointments. The exercises are not difficult but they are daily, for weeks. Patients who follow through generally see the changes the literature describes. Patients who do not often find the release alone produces less than they hoped.
How Dr Depen approaches tongue tie as part of a structural assessment.
Tongue tie sits inside the Jawthodontics™ framework, not outside it. Release is one step in a protocol that may also include jaw expansion (the WideSmiles™ method), myofunctional therapy, and occasionally airway-focused interventions.
The right sequence depends on the structural picture. In adults with significant arch narrowing, expansion may precede release so the tongue has somewhere to go. In others, release and rehabilitation are enough. The £350 Jaw & Airway Analysis is how we decide.

Can you get tongue tie release on the NHS as an adult?
NHS provision for adult tongue tie procedures is inconsistent across England. Many Integrated Care Boards have explicit policies restricting funding to neonatal cases. Adults typically need to self-fund. It is worth checking your local ICB guidance, but the realistic route is private.
Who is a good candidate for adult tongue tie release?
Adults whose tongue cannot elevate adequately, whose symptoms cluster around tongue posture and airway, and whose jaw structure has the room (or can be given the room) to support a corrected tongue posture. Suitability is assessed individually, not by checklist.
Adults whose presenting symptoms are unlikely to trace back to the frenum (for example, isolated speech concerns where myofunctional therapy alone may suffice) may not benefit meaningfully from release. We will say so if that is what the assessment shows.
The next step if you think tongue tie is part of your picture.
Tongue tie in adults cannot be responsibly evaluated without understanding jaw width, tongue space and airway volume. The £350 analysis is the minimum viable starting point. A £25 pre-consultation alone would not give you (or us) the structural picture needed to decide.
Frequently asked
Can you get your tongue tie cut as an adult in the UK?
Yes, adult tongue tie release is available in the UK, though NHS provision is very limited and often restricted to neonatal cases by local commissioning policies. Most adults seeking release will need to self-fund through a private dental or medical provider. A structural assessment beforehand can help determine whether release is appropriate for your specific anatomy.
Is it worth getting a tongue tie release as an adult?
For many adults, release can improve tongue mobility, which may support better tongue posture, jaw function and breathing patterns over time. Release alone is often insufficient: myofunctional rehabilitation is usually recommended alongside the procedure to retrain the tongue's resting position. Whether it is worth it depends on your individual structural picture.
Can you get tongue tie cut on the NHS as an adult?
In most parts of England, NHS funding for adult tongue tie procedures is not routinely available. Some Integrated Care Boards have explicit policies restricting provision to infants. Adults are generally advised to seek private assessment and treatment.
Is tongue tie linked to ADHD?
Some practitioners and researchers have noted associations between restricted oral function, mouth breathing and sleep-disordered breathing, which may in turn affect concentration and behaviour. A direct causal link between tongue tie and ADHD has not been established in robust clinical evidence. If you or your child has both concerns, a structural airway assessment may help clarify whether breathing is a contributing factor.
What happens if tongue tie is left untreated in adults?
Untreated tongue tie in adults may contribute to ongoing low tongue posture, which can affect jaw function, airway volume and breathing patterns. Some adults adapt without significant symptoms; others experience jaw tension, speech difficulty or disrupted sleep that traces back to restricted tongue function. The impact varies considerably between individuals.
How long does recovery from adult tongue tie release take?
Recovery typically involves some soreness and restricted movement for several days following the procedure. Most adults return to normal eating and speaking within one to two weeks, though this can vary depending on the method used and the extent of the release. Myofunctional exercises are usually introduced shortly after the initial healing period.
Does tongue tie affect jaw development in adults?
In adults, jaw development is largely complete, so the direct developmental impact is less than in children. Tongue posture continues to influence jaw joint loading, airway patency and muscle balance throughout life. Correcting tongue posture through release and rehabilitation may support better structural function even in adulthood.