Palatal Expander What it does, & why your jaw width matters more than your teeth.
Most people searching "palatal expander" think they are looking for an orthodontic appliance. What they actually need to understand is that a narrow palate is a structural problem that compresses the airway. Expanding it can change how you breathe, sleep and feel, not just how your teeth sit.
The narrow palate problem most people do not know they have.
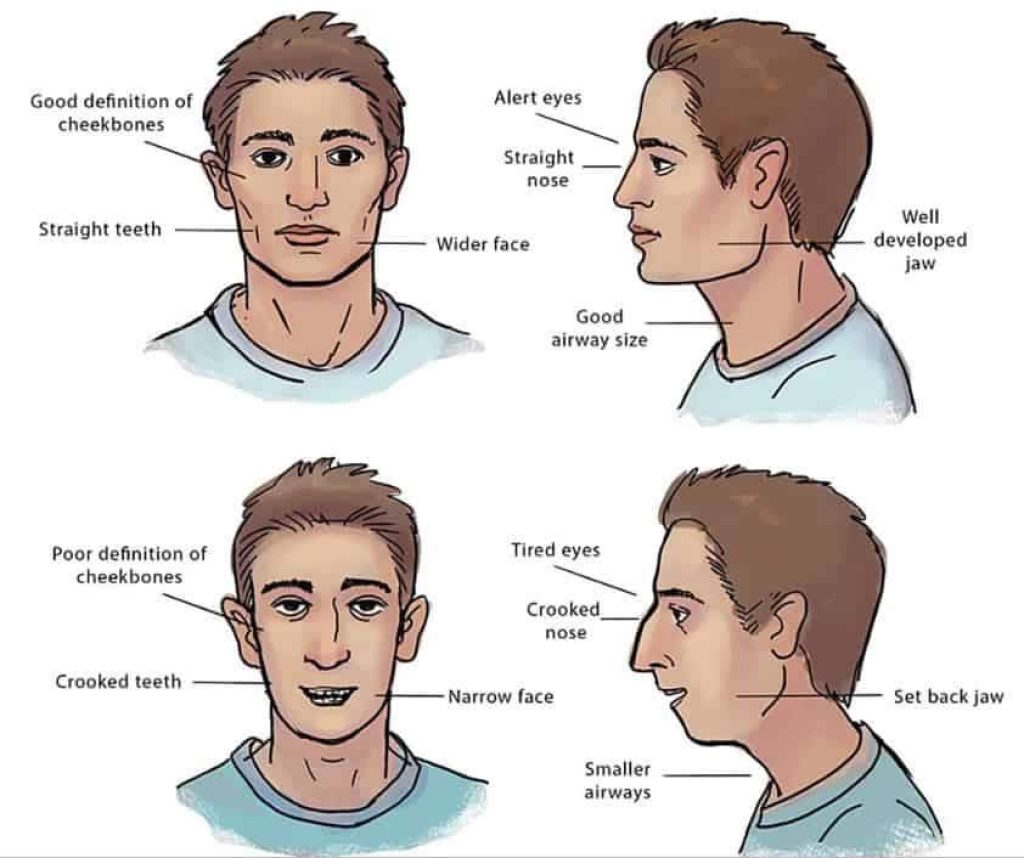
A narrow palate is increasingly common in modern populations. Softer diets, reduced breastfeeding in infancy, and habitual mouth breathing during childhood all reduce the developmental pressure a jaw needs to grow fully. The visible result is often crowded teeth. The structural result is reduced tongue space and a reduced nasal airway above.
Most people with a narrow palate do not realise they have one. It does not hurt. It quietly shapes how the tongue rests, how the airway behaves at night, and how the lower face is supported during the day.
What a palatal expander does inside your mouth.
The device applies controlled lateral force at the mid-palatal suture, the join along the middle of the upper jaw. The two halves of the palate gradually separate and new bone fills the gap. This is bone remodelling, not just tooth movement.
A small diastema (gap) between the upper front teeth often appears during active expansion. It is a sign the suture is opening, not a problem, and it typically closes on its own as the surrounding teeth and bone settle.
The types of palatal expander, and how they differ.
- Removable expanders. Plates and small appliances suitable for younger children with very compliant biology.
- Fixed rapid palatal expanders (RPE / RME). Banded or bonded to the upper teeth and worked on a defined activation schedule. Common through adolescence.
- Bone-anchored devices (MARPE). Titanium miniscrews drive expansion force directly into the palatal bone, bypassing the teeth. Often the only way to achieve meaningful adult skeletal expansion without surgery.
- SARPE. Surgically Assisted Rapid Palatal Expansion. Reserved for cases where the suture is fully fused and non-surgical expansion is not viable.
Why narrow palates are so common now.
The pattern is increasingly recognised in clinical literature: jaws have been getting smaller over the last few generations, faster than genetics can explain. The drivers are environmental, and several of them happen in early childhood before anyone is paying attention to jaw development.
Softer modern diets reduce the chewing load that stimulates jaw growth. Reduced or absent breastfeeding affects early structural signals. Childhood mouth breathing, often linked to allergies or chronic nasal congestion, leaves the tongue resting low instead of against the palate, which removes the natural upward developmental pressure that helps maintain palate width. A narrow palate is rarely a single cause; it is usually the accumulated result of several of these factors.
Saying this is not blame. Most of the factors were normal and unavoidable. It is the reason structural expansion is increasingly relevant for a population that did not historically need it.
Does age matter? What adults need to know.
Yes and no. The mid-palatal suture fuses in adulthood, typically in the mid-to-late twenties with significant variation between individuals. That fusion changes which devices will work, but it does not close the door entirely.
MARPE and surgically-assisted approaches both exist for adults. The right option depends on suture status (assessed with CBCT imaging), bone density, airway picture and goals. Age alone is rarely the deciding factor.

The symptoms a narrow palate can contribute to.
- Crowded upper teeth, or teeth that needed extracting to fit.
- Mouth breathing during the day or on waking.
- Snoring and disrupted sleep.
- Grinding (bruxism) and jaw clicking.
- Tongue-tie tension or a tongue that scallops at the edges.
- Persistent low-grade fatigue, forward head posture, a sense of a recessed lower jaw.
What traditional orthodontics often misses.
Extraction-based orthodontics removes teeth to create room within a narrow arch and retracts the remaining teeth back into the gap. It is fast and produces straight-looking front teeth.
It also reduces the perimeter of the arch and tends to leave the dentition further back than it started. We are not suggesting it is always wrong. We are suggesting it is rarely a complete answer when a narrow upper jaw and a compromised airway are both in play.
How Dr Depen approaches palatal expansion in London.
Jawthodontics™ is the category, and WideSmiles™ is the expansion method we use inside it. Assessment starts with structure and airway, not just tooth alignment. A CBCT scan, an airway and tongue review, and a clinical history are the standard pieces.
The protocol leans slow rather than aggressive. Where appropriate, MARPE is used for adult cases. Where slow expansion can achieve the same result with less invasiveness, slow expansion is used. The device is chosen to fit the case, not the other way around.
What to expect during and after expansion treatment.
Active expansion typically runs over several months, with the device activated on a defined schedule. A retention phase follows to allow the new bone in the suture to consolidate.
Day to day, most patients describe pressure rather than pain, particularly in the first day or two after each adjustment. A temporary gap between the upper front teeth is normal. Speech may feel different for a few days after fitting. None of this is unusual.
What a fitting appointment is actually like.
The fitting appointment for a fixed palatal expander runs around an hour. The teeth are cleaned, the appliance is checked against your individual model, and the device is bonded or banded in place. For MARPE cases in adults the miniscrews are placed first under local anaesthetic, and the expander attaches to them. None of this involves drilling teeth or cutting tissue.
You leave with the device fitted, a small key (for fixed expanders that you activate at home), and written instructions for the activation schedule and aftercare. For the first few days speech can feel slightly different and eating takes some getting used to. Most patients report that by the end of the first week the device feels unremarkable.
Is a palatal expander available on the NHS?
Expansion for children may be available on the NHS in some orthodontic pathways, depending on clinical need. Adult expansion and airway-focused treatment are typically not. Private assessment is usually the route for adults or for anyone wanting a structural diagnosis.
A note for parents researching for a child.
About half the readers of this page are parents who have been told their child needs a palatal expander. The decision is often presented as straightforward; in practice it has more nuance than the leaflet suggests.
The right age for expansion is rarely a single number. The window between roughly seven and twelve years old is often clinically favourable because the mid-palatal suture is responsive and the rest of the face is still developing. Within that window, the right timing for your specific child depends on their bite, their breathing pattern, any tongue tie, and the rate at which their dental development is progressing. Earlier is often better than later, but starting too early in a child who would respond well to slower observation is its own mistake.
A second opinion is reasonable if the first conversation feels rushed. A structural assessment looks at more than the bite, and a clinician who only looks at the teeth is answering a smaller question than the one you came in with. We assess children in the same framework as adults, with imaging and an airway review built in.
Frequently asked
What does a palatal expander do?
A palatal expander applies gentle lateral pressure to the upper jaw, gradually widening the bony arch by encouraging new bone to form along the mid-palatal suture. This can create more space for the tongue, widen the nasal airway, and reduce crowding. The effect is structural, not just cosmetic.
Can adults get a palatal expander?
Adults can often still benefit from palatal expansion, though the approach may differ from childhood treatment. Once the mid-palatal suture has fused, a bone-anchored device such as MARPE may be used to achieve expansion without surgery. The right option depends on your age, anatomy and what a structural assessment reveals.
How long does palatal expansion take?
Treatment duration varies depending on the type of expander, the amount of expansion needed, and the individual's biology. Active expansion may take several months, followed by a retention phase to allow new bone to consolidate. Your clinician can give a more specific estimate after assessment.
Is a palatal expander painful?
Some pressure and mild discomfort are common after each activation, particularly in the first day or two. Most people describe it as a feeling of tightness rather than sharp pain. Discomfort typically settles quickly and can usually be managed with over-the-counter pain relief if needed.
Is palatal expansion available on the NHS?
Palatal expansion for children may be included in some NHS orthodontic treatment plans, depending on clinical need and local commissioning. For adults, and for anyone seeking airway-focused or structural assessment, NHS provision is generally not available and private treatment is the usual route.
What is the difference between a palatal expander and braces?
Braces move teeth within the existing jaw structure. A palatal expander widens the jaw itself, creating more room before or alongside tooth alignment. The two are sometimes used together, but expansion addresses the underlying structural cause of crowding rather than repositioning teeth to fit a narrow arch.
Will I have a gap between my front teeth during treatment?
A temporary gap between the upper front teeth is a normal and expected sign that the mid-palatal suture is opening. This gap typically closes on its own as the surrounding teeth and bone settle, though your clinician will monitor this throughout treatment.