Palate Expander London Widening the jaw to open the airway, for children and adults in Marylebone.
Most people searching for a palate expander in London have already been told their teeth are crowded, their breathing is poor, or their sleep is broken. Nobody has connected those problems to the size of the jaw that holds the tongue. This page does.
Why a narrow palate causes more than crowded teeth.
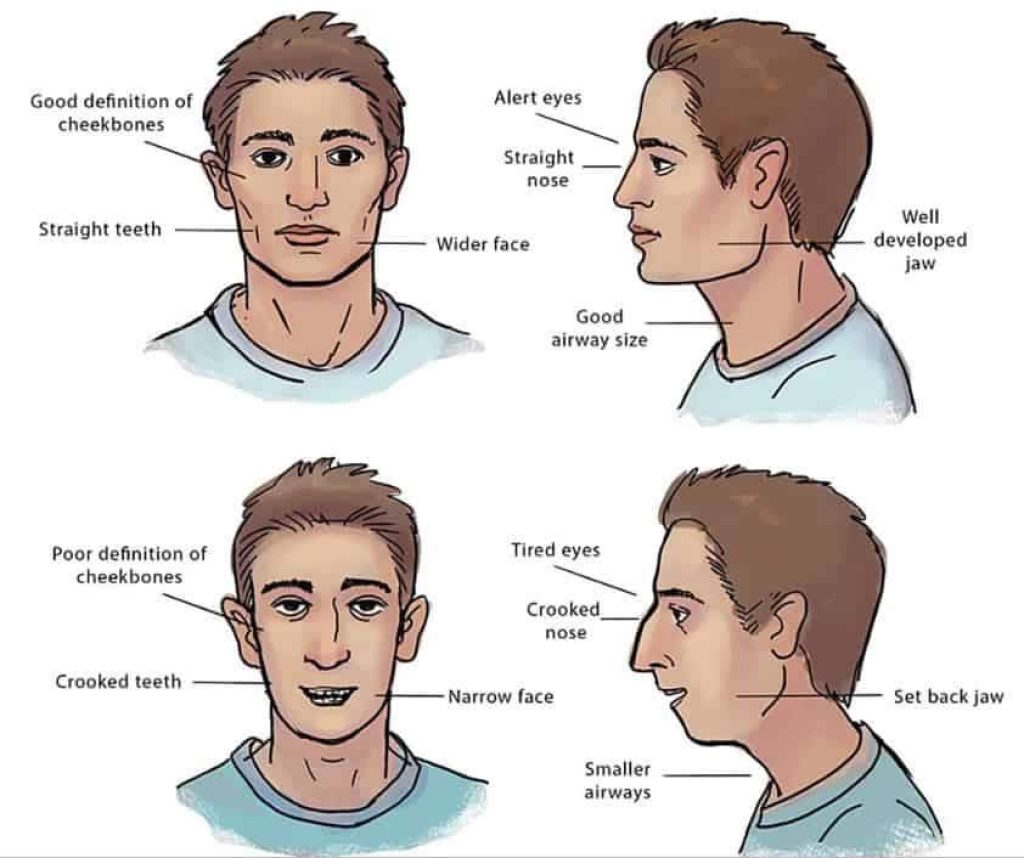
The roof of the mouth is the floor of the nose. A narrow upper arch reduces the space available for the tongue to rest against the palate, which often pushes the tongue back and down, restricting the airway at night and contributing to mouth breathing during the day.
The symptoms that follow are familiar in the clinic: snoring, fatigue that sleep does not fix, jaw clicking, grinding, broken sleep, a feeling of facial compression. None of these are diagnostic on their own. Together they are a structural cluster worth taking seriously.
What a palate expander actually does inside your mouth.
A palate expander is not a brace that pushes teeth. It applies controlled lateral force at the mid-palatal suture, the join along the middle of the upper jaw, encouraging the two halves of the palate to widen as new bone forms in the gap. It is skeletal work, not tooth movement.
The visible signs during treatment can be unsettling if you are not warned: a small gap may appear between the upper front teeth as the suture opens. That diastema is the mechanism working. It typically closes on its own as the surrounding teeth and bone settle.
Children, teenagers, and adults: how age changes the approach.
The mid-palatal suture fuses gradually through adolescence and into early adulthood, with significant individual variation. Childhood expansion is usually quicker because the suture is still open and responsive. Adult expansion is still possible but the appliance, the force protocol and the timeline are all different.
MARPE (Miniscrew-Assisted Rapid Palatal Expander) is the most common bone-anchored option for adults. It applies expansion force directly to the palatal bone via small titanium screws, which is what often allows meaningful adult skeletal change without surgery. Surgically assisted approaches are reserved for the small number of cases that genuinely require them.
The outdated alternative: why extraction often makes the problem worse.
The traditional answer to crowding has been extraction and retraction: remove premolars, pull the remaining teeth backward into the gap. It is fast and produces straight front teeth.
It also reduces the perimeter of the arch, takes space away from the tongue, and tends to leave the soft palate further back than it started. We are not saying every extraction case causes harm. We are saying the airway should be in the room when the decision is made.
How Dr Depen approaches palate expansion in London.
Jawthodontics™ is the category we work in, and WideSmiles™ is the expansion method inside it. The shorthand: structure first, airway always, teeth last. Treatment plans are built around your suture maturity, your airway measurements and your jaw relationship, then around which device delivers the force the bone actually needs.
The protocol leans toward slow expansion that works with biology rather than against it. Where appropriate, we collaborate with myofunctional therapists, sleep doctors and ENT colleagues. The goal is not to win a faster timeline; it is to produce a stable result that holds.

The team and the coordinated-care network in London.
Structural expansion rarely sits in isolation, and the London context lets us coordinate properly with practitioners we know and trust. Myofunctional therapists, sleep doctors, ENT consultants, paediatric airway specialists, and (for children) developmental health practitioners are all part of the broader network we work with.
Where adjunct care is part of the plan, we say so before treatment begins, and where possible we coordinate referrals directly. You should not have to construct your own team out of the internet.
What to expect: timeline, appointments, and what you will feel.
Active expansion typically runs over several months, with the device activated on a defined schedule. A retention phase follows to allow the new bone in the suture to consolidate. Skipping retention is the single most common reason expansion results relapse, which is why we plan it from the start.
Day to day, most patients describe pressure rather than pain. A temporary gap between the upper front teeth is normal during active expansion. Speech may feel slightly different for the first few days after fitting. None of this is unusual and most of it settles within a fortnight.
Visiting the Marylebone clinic.
The clinic is at 1 Orchard Street in Marylebone, a short walk from Bond Street, Marble Arch and Selfridges. Appointments are by booking only, including evenings on request to fit around working schedules. We see patients from across London, the home counties and further afield; travelling for the assessment and major appointments and monitoring more locally where possible is a workable pattern for some adult cases.
Parking is restricted; most patients arrive on foot or by tube. We will confirm the practical details before your appointment so the first visit is unhurried.
A note about London-specific options.
London concentrates a relatively small number of clinicians offering airway-focused jaw expansion in a city of millions. Several factors make the practical landscape narrower than the population would suggest. Most NHS orthodontic provision is tied to paediatric criteria and is not airway-focused. Most private orthodontic practices are alignment-led, with extraction-based treatment still common. The number of London clinics offering bone-anchored adult expansion is small enough to count.
We are stating this because the assumption that London "must have someone" doing what you are looking for is reasonable but not always accurate. The pool is finite. Asking the right questions of any provider, regardless of which clinic, is what protects you from booking with the wrong one.
For patients travelling into London from further afield, the Marylebone clinic is centrally accessible and major appointments can be planned in clusters where helpful. We have patients who travel from outside the M25 for the assessment and active phases, and we will be honest if your geography makes a closer provider a more sensible choice.
A note for parents of London children.
Parents researching options for a child often arrive having been told the NHS route exists but the waiting list is long, or that the case sits on the borderline of IOTN eligibility. London-specific waiting times vary by Integrated Care Board and have generally lengthened over the last few years.
The structural question for a child is rarely just about straight teeth. A narrow palate in a seven- or eight-year-old, particularly one already mouth-breathing or snoring, is a developmental window that does not stay open indefinitely. Earlier intervention is often easier biologically, and a child whose jaw widens during growth tends to integrate the result more naturally than a teenager or adult would.
We see children alongside adults in the same airway-first framework, scaled appropriately. A private structural assessment for a child is similarly bounded and honest: if the case does not warrant intervention yet, we will say so and review in a year rather than start treatment for the sake of starting. The right answer for some London families is "not yet". The right answer for others is "we should not have waited this long".
For families balancing the assessment decision against ongoing NHS waiting lists, the practical question is usually one of timing rather than choice. A private structural assessment costs £350 and gives a clear answer regardless of what happens on the NHS pathway afterwards. Many families use it to clarify whether to keep waiting, to escalate the NHS conversation with better information, or to proceed privately. The assessment is bounded; the implications are yours to decide.
Common questions from London patients before they book.
Adult palate expansion is not routinely available on the NHS in London, and a referral is not required to book a private assessment. Most patients self-refer after recognising the structural picture in something they have read or seen online.
The clinic is in Marylebone, a short walk from Bond Street and Marble Arch. The first appointment is the £350 Jaw & Airway Analysis, which includes the CBCT scan, the airway review and an unhurried conversation. It is fully redeemable against treatment if you decide to proceed.
Is a palate expander right for your jaw? The next step.
Whether expansion suits your specific anatomy is a diagnostic question that imaging settles. The analysis costs £350. The answer is yours regardless of whether you proceed with treatment.
Frequently asked
Can adults get a palate expander in London?
Yes. Adult palate expansion is possible, though the approach often differs from childhood treatment. In adults whose mid-palatal suture has fused, a miniscrew-assisted device such as MARPE may be used to achieve controlled widening. A structural assessment with CBCT imaging can determine whether your jaw is a suitable candidate.
How long does palate expansion take?
The active expansion phase varies considerably depending on age, bone density and the amount of widening needed. Many patients complete the expansion phase over several months, followed by a retention period to allow the new bone to stabilise. A personalised timeline follows the assessment.
Is a palate expander available on the NHS?
Adult palate expansion is not routinely available on the NHS. For children, NHS orthodontic treatment may include expansion in some cases, depending on clinical need and regional waiting lists. Private assessment is typically the most direct route for adults seeking this treatment in London.
Will a palate expander help with snoring or sleep problems?
A narrow upper jaw can reduce the space available for the tongue, which may contribute to airway restriction and snoring during sleep. Widening the arch may help create more tongue space and improve airway patency in some patients. Whether expansion is appropriate for your specific situation depends on a structural and airway assessment.
Does a palate expander hurt?
Most patients describe pressure rather than sharp pain, particularly in the days following an adjustment. A temporary gap between the upper front teeth is normal during active expansion and typically closes as treatment progresses. Discomfort is generally mild and manageable.
What is the difference between a palate expander and traditional braces?
Braces move individual teeth within the existing arch. A palate expander widens the arch itself by stimulating new bone growth at the mid-palatal suture. The two approaches address different structural problems and are sometimes used together as part of a broader treatment plan.
How do I know if my jaw is too narrow?
Common signs include crowded teeth, a high vaulted palate, mouth breathing, tongue scalloping (indentations along the sides of the tongue), and poor sleep quality. A structural assessment that includes arch measurement and airway review is the most reliable way to evaluate whether expansion may be appropriate.