Palate Expander What it actually does, & why it matters beyond your teeth.
Modern jaws are often too narrow to house the tongue comfortably, and a palate expander is one of the structural tools used to address that. This page explains what an expander does to bone and airway, not just to teeth, so you can judge whether it applies to your situation.
The problem most people are not told about.
A narrow palate is not a cosmetic or spacing issue. The roof of your mouth is the floor of your nose. When it is narrow, nasal airflow is often reduced, the tongue has less room to rest correctly, and the airway can be compromised.
The symptoms cluster predictably. Mouth breathing, snoring, crowded teeth, jaw clicking, grinding, broken sleep. None of these is a diagnosis. Together they describe the structural pattern this device exists to address.
What a palate expander is and how it works.
A palate expander is an appliance that applies gentle, controlled force to the mid-palatal suture, the join along the centre of the upper jaw. The two halves of the palate are encouraged to separate, and new bone fills the gap as the body remodels. This is a structural intervention, not a brace that pushes teeth.
Devices fall into two broad categories. Fixed expanders are bonded or banded in place and work continuously. Removable plates can be taken out and depend on the patient remembering to wear them. For older teenagers and adults whose suture has fused, bone-anchored variants (notably MARPE) deliver force directly into the bone via small titanium miniscrews.
The mid-palatal suture: why timing and age matter.
The suture fuses progressively through adolescence and into early adulthood, with significant individual variation. In children, expansion is straightforward because the suture is still open. In adults, the suture is partially or fully fused, which changes the approach.
This is where bone-anchored devices become relevant. They allow meaningful skeletal change after fusion in many adults. Surgical SARPE is reserved for cases where the suture is fully and densely fused and non-surgical expansion is not viable.
There is no single age at which expansion becomes impossible. There is, however, a sliding scale of difficulty. A nine-year-old responds within weeks. A nineteen-year-old often responds within months with a fixed appliance. A thirty-nine-year-old may need a bone-anchored device and a longer timeline, but the underlying biology still permits skeletal change in many cases. The textbook age ranges in clinical literature are guides, not verdicts.
Palate expanders for adults: what has changed.
A decade ago, adults with narrow palates were generally told extraction-based orthodontics was the answer or that nothing could be done. That position has narrowed considerably. MARPE and other bone-anchored protocols have made non-surgical adult expansion realistic in many cases, although not every adult is a candidate and individual assessment remains essential.
The reason this matters is sequencing. An adult patient whose airway and tongue space are the underlying issue benefits very little from straightening teeth in a narrow arch. Addressing the structure first changes the foundation everything else sits on.
The honest version of adult expansion includes its limits. The bone has to be of sufficient density to hold the miniscrews of a MARPE device. The suture has to retain enough biological activity to remodel under load. Severe periodontal disease, very thin palatal bone, or anatomical features that make safe miniscrew placement impossible all rule someone out. A proper assessment will tell you, plainly, if you are in that group.

The outdated approach: extraction and retraction.
For most of the twentieth century, the standard orthodontic answer to a crowded upper arch was to remove premolars and retract the remaining teeth into the gap. It produces straight front teeth fast and remains the default in many practices.
It also reduces the perimeter of the arch, takes space away from the tongue, and pulls the dentition back from the airway. We are not saying every extraction case causes harm. We are saying the airway should be a consideration when the decision is made.
What palate expansion can and cannot do.
Expansion may improve nasal breathing in some cases, create room for the tongue to rest against the palate, reduce crowding, and support better jaw joint function. It is not a cure for sleep apnoea on its own. It is not guaranteed to resolve snoring. Outcomes depend on individual anatomy, age, and how the treatment is planned and monitored.
We are stating limits clearly because the corner of the internet that markets palate expansion often does not. The work is honest mechanism, not a transformation product.
Modern jaws are smaller than our ancestors'. Jaw expansion aims to put nature back on track.
What we actually look at on the CBCT scan.
A CBCT (Cone Beam Computed Tomography) scan is the diagnostic tool that turns "I think your palate is narrow" into a measured answer. It is not the same as a standard dental X-ray. It produces a low-dose three-dimensional reconstruction of the upper jaw, the nasal cavity, the airway and the surrounding bone.
On the scan we measure: suture maturity (whether the join between the two halves of the palate is open, partially fused, or fully fused), palatal bone density and thickness (which determines whether MARPE miniscrews can be safely placed), arch width at several landmarks, nasal cavity volume above the palate, and the dimensions of the pharyngeal airway from the soft palate downward. We also check the relationship between the upper and lower jaws and the position of the jaw joints.
The conversation that follows the imaging is the real value. A scan without interpretation is just pictures. The interpretation is what tells you whether expansion is appropriate, what type of device the bone will tolerate, and what timeline is realistic for your specific anatomy.
How long do the results last?
Expansion results can be stable long-term when treatment is followed by an appropriate retention phase. The new bone that forms in the opened mid-palatal suture takes longer to mature than the visible movement takes to complete. If retention is skipped or shortened, some relapse is common.
In our experience, the cases that hold best combine three things: a properly planned expansion (right device, right rate, right amount), a retention phase that respects the bone biology (months, not weeks), and where indicated, myofunctional support so the tongue learns to rest in the new space it has been given. The tongue is what holds the result in place day to day.
We will not promise lifetime stability. Bone changes throughout adult life and habits change with it. What we will promise is that retention is planned from the start, not as an afterthought when the appliance comes off.
What goes wrong when expansion is skipped.
The most common consequence of skipping expansion in a structurally narrow jaw is not dramatic. It is gradual. Crowding is "fixed" with extractions and retraction, the teeth end up straight, and the structural problem remains untreated. Twenty years later the same patient often presents with broken sleep, jaw clicking, or a sense that something has been off for a long time.
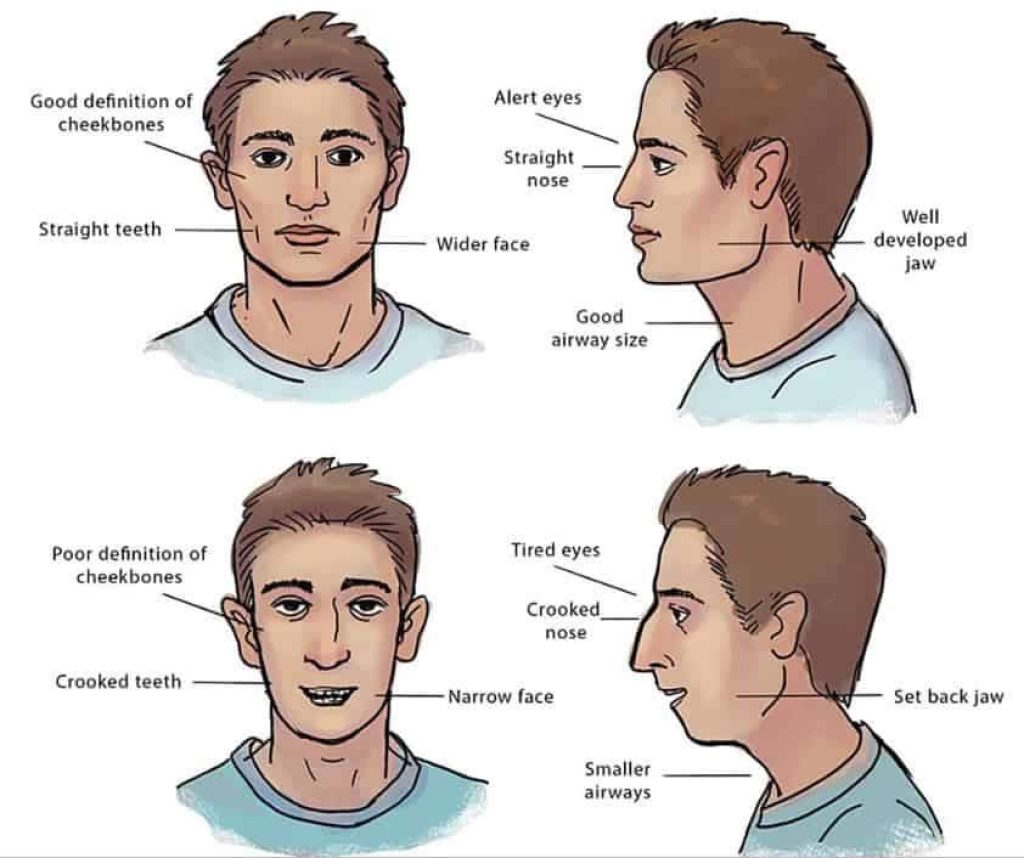
The second consequence is harder to see because it is what did not happen. The jaw did not finish developing. The tongue did not get the room it needed. The airway did not gain the volume it could have. Patients who had expansion at age nine and patients who did not, comparing their faces at thirty, often look like two different people in profile. We are stating this without exaggeration; it is the pattern we see at the clinic.
None of this is a guarantee that expansion would have solved every downstream issue. It is the reason an honest conversation about expansion, at the right age, is more useful than the standard orthodontic offer of "let's see if you grow out of it".
Why we will say no to some patients.
A clinic that says yes to everyone is a clinic that does not look closely enough. We say no, plainly, in several situations: when the CBCT scan shows the suture and bone are not amenable to non-surgical expansion in an adult, and the realistic option is SARPE or no expansion at all; when the airway picture suggests sleep-disordered breathing that needs a sleep doctor first, not an expander first; when the presenting symptoms are unlikely to trace back to jaw width at all and the right answer is to refer onward rather than treat in-house.
In children, we say no when the case does not warrant intervention yet, even if a parent has arrived expecting an appliance. "Watchful waiting" is sometimes the correct answer for a six-year-old whose jaw is developing normally, and the most useful thing we can do is reassure and review in a year.
The honest reason for any of these "no" answers is the same: we want patients who need the work, not patients who can be persuaded into it. If you arrive at our clinic and walk out without a treatment plan, that is the system functioning as it should.
Palate expanders on the NHS: what you need to know.
NHS orthodontic treatment is available for children under 18 in cases that meet the threshold of the Index of Orthodontic Treatment Need (typically grade 4 or 5). Access varies by region and waiting lists are inconsistent.
Adult expansion, particularly MARPE and structural airway-focused treatment, is almost universally a private treatment in the UK. We are stating this without editorialising; it is the practical reality.
What a structural assessment looks like at Dr Depen's clinic.
A CBCT scan to map the suture and airway. A tongue-posture and breathing-pattern review. A jaw joint examination. A conversation about the symptoms that brought you in and the history that explains them. Sixty minutes, £350, fully redeemable against treatment.
Jawthodontics™ is the category we work within, and WideSmiles™ is the expansion method we use. The goal of the analysis is to understand the cause before recommending any device.

Is a palate expander right for you?
Signs worth taking seriously include chronic mouth breathing, a visibly narrow dental arch, a history of teeth removed for orthodontic reasons, snoring or broken sleep, and jaw clicking. None of these is a diagnosis on its own. They are a cluster worth a structural conversation.
The £25 pre-consultation is the right next step for someone in research mode. The full £350 analysis is the right next step for someone ready for clinical answers.
If you are reading this far down the page, the structural argument has either landed for you or it has not. Either is a useful answer. The clinic exists to treat patients whose jaws need the work. If yours does not, an honest assessment will say so, and you will have spent the price of two coffees on a virtual call that saved you from spending more on the wrong treatment elsewhere.
Frequently asked
What does a palate expander do?
A palate expander applies controlled force to the mid-palatal suture, encouraging the two halves of the palate to widen gradually. This may create more space for the teeth and tongue, and can in some cases improve nasal airflow. The effect on breathing depends on individual anatomy and the extent of expansion achieved.
Can adults get a palate expander?
Adults can often benefit from palate expansion, though the approach differs from children's treatment because the mid-palatal suture is typically more fused. A technique called MARPE uses small titanium anchors to apply force at the skeletal level, which may allow meaningful expansion even in adults. A structural assessment is needed to determine candidacy.
Does palate expansion hurt?
Most patients report pressure rather than sharp pain, particularly in the first few days after an adjustment. Some temporary discomfort, mild speech changes and a small gap appearing between the front teeth are common during active expansion. These effects typically settle as treatment progresses.
Is a palate expander available on the NHS?
NHS orthodontic treatment, which may include palate expansion, is available for children under 18 in cases that meet clinical criteria. Adults seeking palate expansion, particularly for airway or structural reasons, will almost always need to pursue private treatment. Waiting lists and eligibility for NHS orthodontics vary by region.
How long does palate expansion take?
The active expansion phase typically lasts several months, followed by a retention period to allow new bone to consolidate. The total timeline varies depending on the device used, the degree of expansion needed and the patient's age. Adult MARPE cases may have different timelines than childhood expansion.
What is the difference between a palate expander and braces?
A palate expander acts on the bone of the palate itself, widening the arch from the inside. Braces move teeth within an existing arch. The two are often used together but address different things. Expansion changes the structural foundation; braces position the teeth within it.
Can a narrow palate affect breathing and sleep?
Because the palate forms the floor of the nasal cavity, a narrow palate may reduce the space available for nasal airflow. This can contribute to mouth breathing, reduced nasal breathing capacity, and in some cases disrupted sleep. Whether expansion will meaningfully improve breathing depends on the individual and requires proper assessment.