Palate Expansion Why the palate is the floor of the airway, and what to do when it is too narrow.
Most people searching "palate expansion" are trying to understand whether a narrow palate is causing their symptoms, not just looking for a definition. The structural view: a narrow palate is not a cosmetic quirk but a space problem that compresses the airway, crowds the tongue, and often drives the symptoms that brought you here.
What a narrow palate actually is, and why so many people have one.
A narrow palate is the developmental result of a jaw that did not widen to its full potential during childhood. Modern lifestyle factors are usually the cause. Softer diets reduce the chewing load that stimulates jaw growth. Reduced breastfeeding affects early developmental signals. Mouth breathing, often linked to allergies or blocked noses, leads to longer narrower facial development.
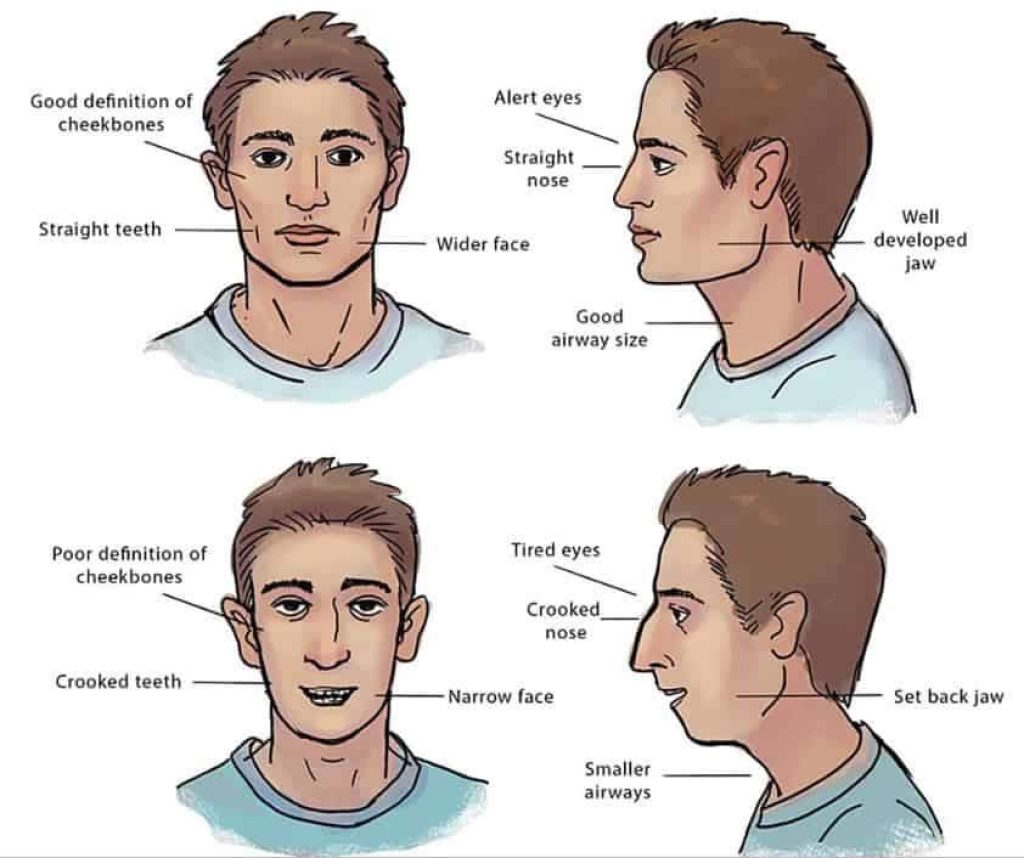
The visible signs in adulthood are crowding, a high-arched palate, and often a face that looks slightly compressed in profile. The hidden signs are reduced tongue space and a compromised airway. The pattern is increasingly common.
The symptoms that often trace back to palate width.
The chain: narrow palate, reduced tongue space, tongue pushed back, airway compressed. The symptoms that follow are familiar in the clinic.
- Snoring and broken sleep that does not refresh.
- Mouth breathing during the day or on waking with a dry mouth.
- Grinding (bruxism) and jaw clicking.
- Crowded teeth or a high-arched palate.
- Forward head posture or a sense of a recessed lower jaw.
None of these is a diagnosis on its own. Together they describe a pattern worth a structural conversation.
How palate expansion works: the biological mechanism.
A palate expander applies controlled lateral force at the mid-palatal suture. The two halves of the palate gradually separate and new bone forms in the gap as the body remodels.
WideSmiles™ is the slow-expansion method we use within the broader Jawthodontics™ framework. Rather than aggressive forces and rapid protocols, slow expansion respects the body's healing capacity in both children and adults. Where appropriate, this avoids surgical routes entirely.

Child versus adult expansion: what is actually different.
In children, the mid-palatal suture is open and responsive. Conventional removable or fixed expanders typically produce real skeletal change. The biology does most of the work.
In adults, the suture is partially or fully fused. Tooth-borne devices alone often tip teeth outward rather than widen the bone. Bone-anchored devices (MARPE/MSE), surgically-assisted expansion (SARPE), and slow-expansion protocols designed for adult biology all exist. The right one depends on individual anatomy.
Why narrow jaws are increasingly common.
The trend is consistent in clinical observation and increasingly documented in the literature: jaws are smaller than they were a few generations ago, faster than genetics can explain. The drivers are environmental.
Softer modern diets reduce the chewing load that stimulates jaw development. Reduced breastfeeding affects early structural signals. Childhood mouth breathing, often linked to allergies or chronic nasal congestion, leaves the tongue resting low rather than against the palate, removing the natural developmental pressure that helps maintain palate width. Each of these factors is normal and largely unavoidable. The cumulative effect is what we see in the clinic.
What palate expansion is not.
It is not extraction-based orthodontics, which removes teeth to create space within an arch that was the wrong size to begin with. It is not retraction-based treatment, which moves teeth backward into the airway. It is not a "wait and see" approach.
It is also not a cure for sleep apnoea on its own. Expansion may improve nasal airway volume and tongue posture, which can support better breathing. It is one piece of a wider picture in airway-driven cases.
Where palate expansion fits in the sequence of treatment.
In an airway-first approach, expansion is usually one of the earlier steps, not the last. The logic is foundational: changing the size of the arch changes what tooth alignment, retention and airway-targeted interventions are possible afterwards. Alignment before expansion often produces straight teeth in an arch that is still the wrong size; that result tends to be cosmetic without being structural.
A typical sequence might run: assessment, expansion, retention, alignment with aligners or fixed appliances if needed, and any adjunct work (tongue tie release, myofunctional therapy, sleep evaluation) at the points where it best supports the overall plan. The order is decided after the imaging, not before.
What a structural assessment actually involves.
Imaging (CBCT), an airway assessment, a tongue-posture review, a jaw joint examination, and an unhurried conversation about your specific symptoms and history. Sixty minutes. £350. Fully redeemable against treatment.
The assessment exists to understand the cause, not to commit you to a device.
What we measure on the CBCT scan.
The scan turns "your palate looks narrow" into measured anatomy. We assess suture maturity (open, partially fused, fully fused), bone density and thickness at any planned miniscrew sites, root proximity, arch width at several landmarks, nasal cavity volume above the palate, and the dimensions of the pharyngeal airway. We also check the jaw joints.
The conversation that follows the measurements is what makes them useful. A scan without interpretation is just pictures. The interpretation is what tells you whether expansion is appropriate, what type of device the bone will tolerate, and what timeline is realistic.
What happens after expansion: the alignment phase.
Expansion changes the size of the arch. It does not, on its own, finish positioning the teeth within the new arch. Most cases (adult and child) involve an alignment phase after expansion is complete and the suture has consolidated.
For adults this is often a course of clear aligners. For children it may be a shorter phase of orthodontic alignment timed with ongoing facial growth. The alignment phase is usually shorter and simpler than alignment without expansion would have been, because the arch is now the right size to house the teeth without crowding.
We will tell you on day one whether alignment is likely to be part of your plan and roughly how long it will run. The total project length, expansion plus retention plus alignment, is usually quoted as a range rather than a date. Biology does not run on a calendar.
Is palate expansion available on the NHS?
Provision is generally limited to children meeting specific clinical criteria (IOTN grade 4 or 5 in most cases), and access varies by region. Adults seeking expansion for structural or airway reasons typically need to pursue this privately.
What to do if you think your palate may be narrow.
Start with the free Jaw Quiz. Two minutes of questions designed to map your symptoms against the structural causes a clinician would explore. It is the lowest-friction way to find out whether a conversation is worth having.
Frequently asked
Can adults have palate expansion?
Yes, adults can often have palate expansion, though the approach differs from childhood treatment. Because the mid-palatal suture may have fused, adult cases often require a miniscrew-assisted device (MARPE) or, in some cases, a surgical procedure. A structural assessment can clarify which option may be appropriate for your specific anatomy.
How long does palate expansion take?
Treatment timelines vary depending on the method used and the degree of expansion needed. Active expansion may take several months, followed by a retention phase to allow new bone to consolidate. Your clinician can give a more specific estimate after reviewing your case.
Does palate expansion help with snoring or sleep problems?
In many cases, a narrow palate contributes to reduced tongue space and a compressed airway, which can be a factor in snoring and disrupted sleep. Expanding the palate may help create more room for the tongue to rest forward, potentially improving airway patency. This is not a guaranteed outcome and depends on the individual case.
Is palate expansion painful?
Most patients report pressure rather than pain during the active expansion phase. Some discomfort is common in the first few days after adjustments. The process is designed to work with the body's natural bone remodelling capacity rather than against it.
Is palate expansion available on the NHS?
NHS palate expansion is generally available only for children who meet specific clinical criteria, and provision varies by region. Adults seeking expansion for structural or airway reasons will typically need to pursue private treatment.
At what age is palate expansion most effective?
Expansion is often most straightforward in children and teenagers, before the mid-palatal suture begins to fuse. Adult expansion is possible using different techniques. There is no single age cut-off, and individual anatomy varies, so a structural assessment is the most reliable way to understand your options.
What is the difference between palate expansion and braces?
Braces move teeth within the existing jaw structure. Palate expansion widens the jaw arch itself, creating more space. Expansion addresses the root cause of crowding rather than managing its appearance. The two approaches are not mutually exclusive and are sometimes used together.