Tongue Tie in Adults The airway problem nobody told you about.
Tongue tie in adults is not a childhood problem that was missed. It is a structural issue that quietly restricts the tongue's resting position, narrows the jaw, and reduces the airway, often for decades before anyone joins the dots.
Most adults with tongue tie were never properly assessed as children.
Tongue tie is frequently dismissed in childhood as mild or cosmetically insignificant. Many adults carry a restriction they were never told would matter later. Posterior (submucosal) ties are particularly likely to be missed on visual inspection.
The point is not blame. It is recognition. The structural consequences accumulate over decades, and they are easier to notice in adulthood than the original restriction was in infancy.
What tongue tie actually does to your jaw and airway.
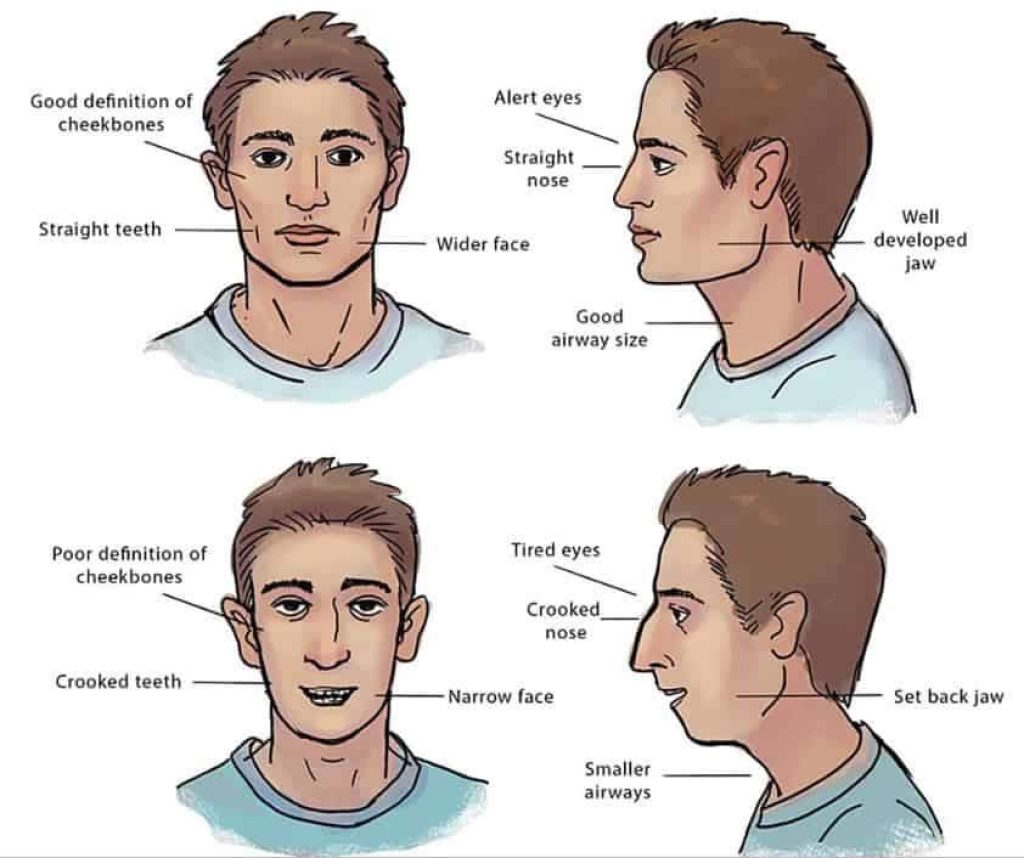
The tongue at rest is meant to sit against the roof of the mouth. That posture provides the upward developmental pressure that helps maintain palate width. A restricted frenulum prevents this. The tongue rests low and forward instead.
A narrow palate means a narrower airway. The anatomical chain runs: frenulum, tongue posture, palatal width, nasal airway volume, pharyngeal airway. Each link affects the next. The symptoms appear at the downstream end and are rarely traced back to the source.
Why classifying tongue tie is harder than it looks.
There is no universally agreed classification system for adult tongue tie. The Kotlow classification and the Hazelbaker Assessment Tool are widely cited but were developed primarily for infant feeding assessment. Coryllos described four anterior-posterior types. Different practitioners use different criteria and the same tongue can score very differently between assessors.
For the structural question that matters here (is the tongue able to reach and rest against the palate), classification alone is insufficient. We assess function: how well the tongue elevates with the mouth open, how far it can extend, whether it can sweep along the palate, what the swallow looks like, and how the tongue sits at rest. The grade matters less than the functional consequences in your specific anatomy.
The symptoms adults describe, and why they are easy to miss.
Many of these symptoms have been individually treated for years before anyone considered them as a cluster. Snoring has been blamed on weight. Jaw clicking on stress. Fatigue on workload. Each explanation is plausible in isolation, which is exactly why the structural cause is so often missed.
- Snoring and disrupted sleep.
- Mouth breathing during sleep or on waking.
- Jaw clicking, tension or grinding.
- Fatigue that sleep does not fix.
- A feeling of a restricted or recessed jaw.
- Difficulty swallowing or speech that feels effortful.
- Dental crowding, often dismissed as cosmetic.
Each of these is routinely attributed to other causes. The structural cluster is rarely named.
Why "just snip it" is rarely the whole answer for adults.
A frenectomy (release) alone, without addressing the structural narrowing that developed over years, often produces limited results. The tongue needs somewhere to go. If the palate is still narrow, releasing the tie does not restore tongue posture or airway volume by itself.
This is why adult release without rehabilitation often disappoints. The anatomy is changed; the function is not. A coordinated plan tends to outperform the cut alone.
What myofunctional therapy actually does.
Myofunctional therapy is the muscular retraining piece that often gets dismissed as "tongue exercises". It is more substantial than that. A qualified myofunctional therapist (in the UK, often a speech and language therapist with additional training) assesses tongue strength, mobility and resting position, and prescribes a programme of exercises designed to retrain the tongue, lips and breathing pattern.
For adults with long-standing tongue tie, this work is essential alongside any release. The muscles have spent decades compensating for restricted movement. Cutting the frenum changes the anatomy in a single appointment; the muscles need months to learn to use the new range of motion. Without the retraining, many patients find the tongue continues to rest in its old low-and-forward position even with a fully released frenum.
We refer to therapists we know and trust. The work happens between appointments, daily, for weeks to months. It is not glamorous and it is not optional in adult cases that warrant release.
The structural approach: expansion first, release second.
Within Jawthodontics™, the sequence often runs in the opposite order to what patients expect. Jaw expansion using WideSmiles™ widens the palate and creates the space the tongue needs. Frenectomy may then be performed with the tongue having room to function in. Myofunctional therapy retrains the function the muscles never had a chance to learn.
This is a coordinated process, not a single procedure. The right sequence depends on the structural picture and is decided after a proper assessment.

Can adults actually expand their jaw? The biology.
Yes, in many cases. Palatal suture remodelling is possible in adults, particularly with controlled, slow expansion protocols and bone-anchored devices where the suture has fused. Age and individual anatomy affect the approach.
A structural assessment with CBCT imaging is the only honest way to know what is possible for your specific anatomy. We will not promise outcomes the imaging does not support.
What the evidence actually says about adult tongue tie.
The clinical literature on adult tongue tie is uneven. There are robust studies on infant feeding outcomes. There is growing literature on the connection between tongue posture, palatal width and airway function in children. The adult evidence base is thinner, and we will not pretend otherwise.
What we can say is what we observe at the clinic. Adults who present with the structural cluster (narrow palate, restricted frenum, mouth breathing, snoring) often improve meaningfully with a coordinated approach that combines expansion, release and myofunctional therapy. The reverse, expecting release alone to resolve symptoms, often disappoints. The pattern is consistent enough that we plan for it.
Outcomes still vary individually, and a careful assessment is what tells us whether your specific case is likely to respond. We will say so if we think it is not.
What you can do today, before any clinical decision.
Three observations are worth making before any clinical conversation. None of them is a diagnosis. All of them sharpen the conversation when you do have one.
First, can you touch the roof of your mouth with the tip of your tongue while keeping your mouth open wide enough to fit two fingers? Many adults with significant tongue tie cannot. Second, when you swallow saliva consciously, does your tongue tip stay against the roof of the mouth, or does it press against the back of your lower teeth or thrust forward? The latter is a sign of a swallow pattern adapted around restricted tongue posture. Third, when you sit at rest reading or working, where does your tongue rest? If you are not sure, it is probably resting low on the floor of the mouth, which is the pattern we expect in tongue-tied adults.
These are useful self-observations to bring to an assessment. They are not a substitute for the assessment itself, but they prime the conversation and they help you notice patterns you may have lived with without noticing. Adults with normal tongue posture and function rarely think about any of this. Adults with restriction often realise they have never actively considered it.
What a tongue tie assessment at Dr Depen's clinic involves.
Structural photographs, airway screening, tongue function assessment (elevation, lateralisation, swallow), and a review of symptoms in the context of jaw size. The goal is to understand the root cause, not to treat the tongue tie in isolation.
The £350 Jaw & Airway Analysis covers all of this. It is fully redeemable against treatment if you decide to proceed.

The next step if you suspect tongue tie is affecting your airway.
There is a lot of conflicting advice in this area. The fastest sensible step is the £25 pre-consultation: a 15-minute virtual call to find out whether the full structural assessment is worth booking. It is not a sales call. Many readers leave with a clearer picture either way.
If you have read this far, the structural argument has either resonated with what you have been living with, or it has not. Either reading is useful. Tongue tie is a small piece of tissue with disproportionate downstream effects when it has been restricting function for decades. The clinical conversation about it deserves to be honest, hedged where the evidence is thin, and specific to your anatomy rather than the general literature.
Frequently asked
Can tongue tie cause problems in adults if it was not treated in childhood?
Yes, it can. In many adults, an untreated tongue tie may contribute to low tongue posture, which over time can be associated with a narrower palate and reduced airway space. Symptoms such as snoring, mouth breathing and jaw tension are often reported, though the degree of impact varies between individuals.
Is it too late to treat tongue tie as an adult?
It is rarely too late to address the restriction itself. A frenectomy can be performed at any age. The structural changes that may have developed over years, such as a narrow palate, often require a coordinated approach that includes jaw expansion alongside or before the release.
What are the signs of tongue tie in adults?
Common signs may include difficulty lifting the tongue to the roof of the mouth, a heart-shaped tongue tip when extended, snoring or disrupted sleep, jaw clicking or tension, dental crowding and a history of mouth breathing. Many adults are unaware they have a restriction until they are assessed by a clinician who looks for it.
Does the NHS treat tongue tie in adults?
NHS provision for tongue tie treatment is largely focused on infants, particularly in relation to breastfeeding difficulties. Adult tongue tie assessment and treatment, especially when approached from an airway or structural perspective, is not routinely available on the NHS and is typically provided through specialist private clinics.
What is the difference between tongue tie release and jaw expansion?
A tongue tie release removes the physical restriction on tongue movement. Jaw expansion widens the palate to create the space the tongue needs to rest and function correctly. In many adult cases, expansion may be recommended before or alongside a release, because releasing the tongue without adequate space can limit the benefit of the procedure.
Can tongue tie affect sleep in adults?
It may. A tied tongue can prevent the tongue from resting against the palate during sleep, which may contribute to the tongue falling back and partially obstructing the airway. This can be associated with snoring and, in some cases, sleep-disordered breathing. The relationship is indirect and varies between individuals.
How do I know if my tongue tie is affecting my jaw or airway?
A standard tongue tie assessment focused on speech will not typically evaluate jaw structure or airway volume. A structural assessment, which looks at palatal width, jaw position and airway screening alongside tongue function, is needed to understand whether the restriction is contributing to broader structural issues.